Decubitus ulcer and pressure injury both refer to localized damage to the skin and underlying tissue caused by prolonged pressure, often occurring in patients with limited mobility. Pressure injuries are classified into stages based on severity, ranging from non-blanchable erythema to full-thickness tissue loss, while decubitus ulcer is a traditional term often used interchangeably. Explore detailed differences, prevention strategies, and treatment options to better understand managing these conditions.
Main Difference
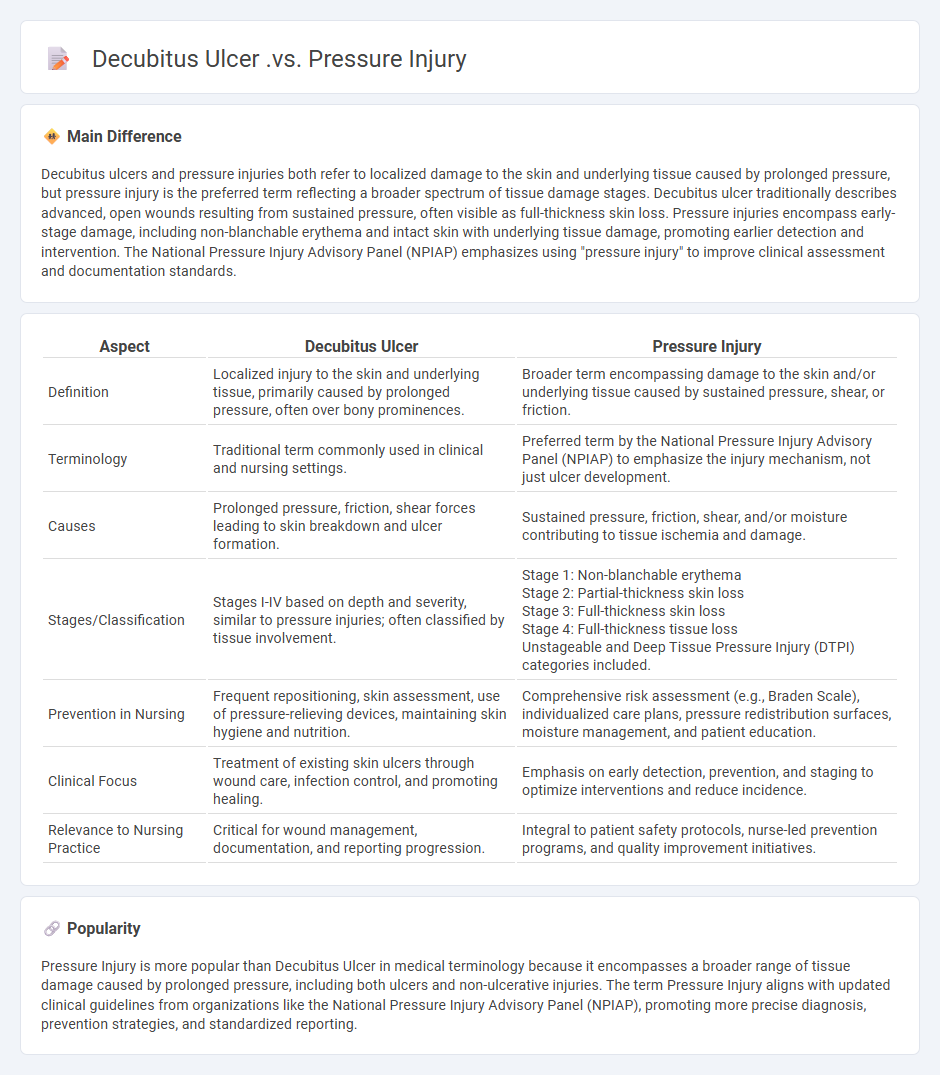
Decubitus ulcers and pressure injuries both refer to localized damage to the skin and underlying tissue caused by prolonged pressure, but pressure injury is the preferred term reflecting a broader spectrum of tissue damage stages. Decubitus ulcer traditionally describes advanced, open wounds resulting from sustained pressure, often visible as full-thickness skin loss. Pressure injuries encompass early-stage damage, including non-blanchable erythema and intact skin with underlying tissue damage, promoting earlier detection and intervention. The National Pressure Injury Advisory Panel (NPIAP) emphasizes using "pressure injury" to improve clinical assessment and documentation standards.
Connection
Decubitus ulcers, also known as pressure ulcers or bedsores, develop due to prolonged pressure on the skin that reduces blood flow, leading to tissue damage. Pressure injuries encompass a broader range of localized damage to the skin and underlying tissue caused by pressure, shear, or friction. Both terms describe conditions resulting from sustained mechanical forces impairing skin integrity, commonly affecting immobile patients in healthcare settings.
Comparison Table
| Aspect | Decubitus Ulcer | Pressure Injury |
|---|---|---|
| Definition | Localized injury to the skin and underlying tissue, primarily caused by prolonged pressure, often over bony prominences. | Broader term encompassing damage to the skin and/or underlying tissue caused by sustained pressure, shear, or friction. |
| Terminology | Traditional term commonly used in clinical and nursing settings. | Preferred term by the National Pressure Injury Advisory Panel (NPIAP) to emphasize the injury mechanism, not just ulcer development. |
| Causes | Prolonged pressure, friction, shear forces leading to skin breakdown and ulcer formation. | Sustained pressure, friction, shear, and/or moisture contributing to tissue ischemia and damage. |
| Stages/Classification | Stages I-IV based on depth and severity, similar to pressure injuries; often classified by tissue involvement. | Stage 1: Non-blanchable erythema Stage 2: Partial-thickness skin loss Stage 3: Full-thickness skin loss Stage 4: Full-thickness tissue loss Unstageable and Deep Tissue Pressure Injury (DTPI) categories included. |
| Prevention in Nursing | Frequent repositioning, skin assessment, use of pressure-relieving devices, maintaining skin hygiene and nutrition. | Comprehensive risk assessment (e.g., Braden Scale), individualized care plans, pressure redistribution surfaces, moisture management, and patient education. |
| Clinical Focus | Treatment of existing skin ulcers through wound care, infection control, and promoting healing. | Emphasis on early detection, prevention, and staging to optimize interventions and reduce incidence. |
| Relevance to Nursing Practice | Critical for wound management, documentation, and reporting progression. | Integral to patient safety protocols, nurse-led prevention programs, and quality improvement initiatives. |
Pressure Ulcer
Pressure ulcers, also known as bedsores or decubitus ulcers, commonly affect patients with limited mobility, particularly those confined to beds or wheelchairs. These wounds result from prolonged pressure that impairs blood flow, leading to tissue ischemia and necrosis, predominantly occurring over bony prominences such as the sacrum, heels, and hips. Effective nursing interventions include regular repositioning, use of pressure-relieving devices, maintaining skin hygiene, and assessing nutritional status to promote wound healing and prevent complications. Advanced care strategies involve wound assessment using standardized tools like the Braden Scale and implementing evidence-based dressing protocols tailored to the ulcer's stage and severity.
Decubitus Ulcer
Decubitus ulcers, commonly known as pressure ulcers or bedsores, are localized injuries to the skin and underlying tissue primarily caused by prolonged pressure, often seen in immobile patients. They frequently develop over bony prominences such as the sacrum, heels, and hips, with prevalence rates in hospitalized patients ranging from 5% to 15%. Effective nursing interventions include regular repositioning every two hours, maintaining skin hygiene, and using pressure-relieving devices like specialized mattresses. Early identification and staging, according to the National Pressure Injury Advisory Panel (NPIAP) guidelines, are critical to preventing complications such as infections and extended hospital stays.
Staging System
The staging system in nursing categorizes disease progression to guide treatment plans and predict patient outcomes effectively. Commonly applied in oncology, such as the TNM (Tumor, Node, Metastasis) system, staging helps nurses assess the severity and spread of cancer, supporting timely interventions. Accurate staging requires thorough patient assessment, including diagnostic tests and clinical evaluation, to document tumor size, lymph node involvement, and distant metastases. This standardized approach enhances communication among healthcare teams and improves personalized care strategies for patients.
Pressure Injury Prevention
Effective pressure injury prevention in nursing includes regular patient repositioning every two hours to reduce prolonged pressure on vulnerable skin areas. Utilizing pressure-relieving devices such as specialized mattresses and cushions minimizes tissue damage risk, particularly in immobile or elderly patients. Nutritional support and skin hydration are critical factors that enhance skin integrity and promote healing. Comprehensive risk assessment tools like the Braden Scale guide individualized care plans to prevent pressure ulcers.
Wound Assessment
Wound assessment in nursing involves a systematic evaluation of wound type, size, depth, tissue type, and the presence of exudate to guide effective treatment. Nurses use standardized tools like the Bates-Jensen Wound Assessment Tool or the Pressure Ulcer Scale for Healing (PUSH) to document wound progress accurately. Accurate wound assessment supports infection control, promotes optimal healing, and reduces complications such as pressure ulcers or chronic wounds. Evidence-based assessment techniques contribute to improved patient outcomes and streamlined care planning in clinical practice.
Source and External Links
Decubitus Ulcers vs. Pressure Ulcers | Nursing Care Center - The term "pressure ulcer" is broader, encompassing any ulcerations caused by pressure (such as from prosthetic limbs), while "decubitus ulcer" specifically refers to skin and tissue breakdown due to prolonged pressure over bony prominences like sacrum or heels.
Pressure Ulcers (Pressure Injuries) - Sepsis Alliance - Pressure ulcers, also known as decubitus ulcers, pressure sores or bed sores, develop from pressure causing skin damage, commonly due to immobility and interrupted blood flow, with potential serious infections including sepsis.
Pressure ulcer - Wikipedia - Pressure ulcers (pressure sores, bed sores, or pressure injuries) are localized damage to skin and tissue usually at bony areas caused by prolonged pressure and/or shear, mostly affecting immobile patients, and the term pressure ulcer is more widely used clinically than decubitus ulcer.
FAQs
What is a decubitus ulcer?
A decubitus ulcer, also known as a pressure ulcer or bedsore, is a localized injury to the skin and underlying tissue caused by prolonged pressure, often occurring over bony prominences in immobile patients.
What is a pressure injury?
A pressure injury is localized damage to the skin and underlying tissue caused by prolonged pressure, often occurring over bony areas such as heels, sacrum, and elbows.
What is the difference between a decubitus ulcer and a pressure injury?
A decubitus ulcer is a type of pressure injury characterized by localized damage to the skin and underlying tissue due to prolonged pressure, while pressure injury encompasses all stages of tissue damage from non-blanchable erythema (stage 1) to deep ulcers (stage 4), including but not limited to decubitus ulcers.
What causes decubitus ulcers?
Decubitus ulcers are caused by prolonged pressure on the skin, leading to impaired blood flow and tissue damage.
What are the stages of pressure injuries?
The stages of pressure injuries are: Stage 1 - non-blanchable erythema of intact skin; Stage 2 - partial-thickness skin loss with exposed dermis; Stage 3 - full-thickness skin loss involving damage or necrosis of subcutaneous tissue; Stage 4 - full-thickness tissue loss with exposed bone, tendon, or muscle; Unstageable - obscured full-thickness skin and tissue loss; and Deep Tissue Pressure Injury - persistent non-blanchable deep red, maroon, or purple discoloration.
How can decubitus ulcers be prevented?
Decubitus ulcers can be prevented by regularly repositioning patients every two hours, maintaining skin hygiene, using pressure-relieving devices like specialized mattresses or cushions, ensuring proper nutrition and hydration, and managing underlying conditions such as diabetes or immobility.
Why is early detection of pressure injuries important?
Early detection of pressure injuries is important because it prevents infection, reduces treatment costs, and improves patient recovery outcomes.