Nociceptive pain arises from actual tissue damage or inflammation, activating pain receptors in skin, muscles, or organs, while neuropathic pain results from nerve damage or dysfunction causing abnormal signal processing in the nervous system. Common examples include arthritis or injury-related pain for nociceptive, and diabetic neuropathy or shingles for neuropathic pain. Explore further to understand distinct treatment approaches and diagnostic criteria for both types of pain.
Main Difference
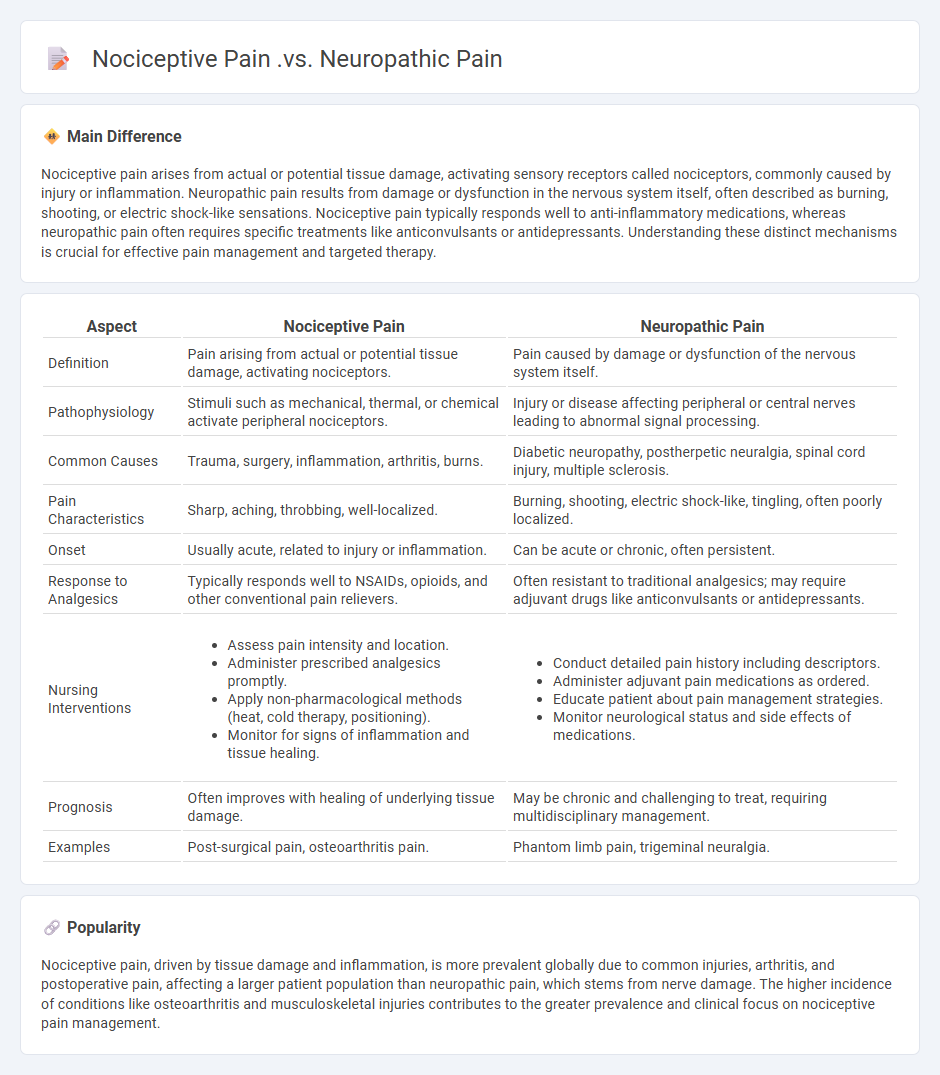
Nociceptive pain arises from actual or potential tissue damage, activating sensory receptors called nociceptors, commonly caused by injury or inflammation. Neuropathic pain results from damage or dysfunction in the nervous system itself, often described as burning, shooting, or electric shock-like sensations. Nociceptive pain typically responds well to anti-inflammatory medications, whereas neuropathic pain often requires specific treatments like anticonvulsants or antidepressants. Understanding these distinct mechanisms is crucial for effective pain management and targeted therapy.
Connection
Nociceptive pain arises from tissue damage activating nociceptors, while neuropathic pain results from nerve injury or malfunction. Both pain types share overlapping molecular pathways, including the involvement of inflammatory mediators and altered ion channel expression. Chronic nociceptive pain can lead to peripheral and central sensitization, increasing the likelihood of developing neuropathic pain components.
Comparison Table
| Aspect | Nociceptive Pain | Neuropathic Pain |
|---|---|---|
| Definition | Pain arising from actual or potential tissue damage, activating nociceptors. | Pain caused by damage or dysfunction of the nervous system itself. |
| Pathophysiology | Stimuli such as mechanical, thermal, or chemical activate peripheral nociceptors. | Injury or disease affecting peripheral or central nerves leading to abnormal signal processing. |
| Common Causes | Trauma, surgery, inflammation, arthritis, burns. | Diabetic neuropathy, postherpetic neuralgia, spinal cord injury, multiple sclerosis. |
| Pain Characteristics | Sharp, aching, throbbing, well-localized. | Burning, shooting, electric shock-like, tingling, often poorly localized. |
| Onset | Usually acute, related to injury or inflammation. | Can be acute or chronic, often persistent. |
| Response to Analgesics | Typically responds well to NSAIDs, opioids, and other conventional pain relievers. | Often resistant to traditional analgesics; may require adjuvant drugs like anticonvulsants or antidepressants. |
| Nursing Interventions |
|
|
| Prognosis | Often improves with healing of underlying tissue damage. | May be chronic and challenging to treat, requiring multidisciplinary management. |
| Examples | Post-surgical pain, osteoarthritis pain. | Phantom limb pain, trigeminal neuralgia. |
Etiology (Cause)
In nursing, etiology refers to the study and identification of the underlying causes of diseases or medical conditions, essential for accurate diagnosis and effective treatment planning. Understanding the etiology enables nurses to tailor interventions based on the origin of symptoms, whether stemming from infectious agents, genetic factors, environmental exposures, or lifestyle choices. Accurate assessment of etiology improves patient outcomes by guiding evidence-based nursing care and prevention strategies. Comprehensive knowledge of disease causation supports holistic nursing practices aimed at promoting health and managing chronic conditions.
Pain Characteristics
Pain characteristics are critical for accurate assessment and effective management in nursing practice. Key attributes include location, intensity, duration, quality, and aggravating or relieving factors, which guide tailored interventions. Nurses utilize standardized pain scales such as the Numeric Rating Scale (NRS) and the Wong-Baker FACES Pain Rating Scale for consistent evaluation. Understanding these characteristics contributes to improved patient outcomes and enhances overall care quality.
Assessment Strategies
Assessment strategies in nursing are critical for collecting accurate patient data and ensuring effective care plans. Techniques such as physical examination, patient interviews, and diagnostic testing help nurses evaluate patient health status comprehensively. Utilization of standardized tools like the Glasgow Coma Scale and Braden Scale enhances consistency and objective measurement during assessments. Continuous assessment allows early identification of complications and timely intervention, improving patient outcomes across various clinical settings.
Treatment Approaches
Effective nursing treatment approaches emphasize patient-centered care, integrating evidence-based practices to address both acute and chronic conditions. Interventions often include medication administration, wound care, patient education, and psychosocial support tailored to individual health needs. Nurses utilize comprehensive assessments and interdisciplinary collaboration to develop personalized care plans that improve patient outcomes. Technological tools such as electronic health records enhance accuracy and efficiency in monitoring treatment progress.
Patient Education
Patient education in nursing empowers individuals to manage their health effectively by providing tailored information on disease prevention, treatment options, and medication adherence. Nurses utilize evidence-based teaching strategies and plain language to enhance comprehension, address cultural differences, and promote health literacy. Effective patient education has been linked to improved clinical outcomes, reduced hospital readmissions, and increased patient satisfaction according to studies published by the American Nurses Association. Integrating ongoing assessment and documentation ensures that educational interventions meet individual needs and support long-term wellness.
Source and External Links
Nociceptive vs Neuropathic Pain: What's The Difference? - Nociceptive pain is caused by physical damage or injury to body tissues, often visible and typically temporary, while neuropathic pain results from damage to the nervous system, is internal, chronic, and often related to underlying illness.
Nociceptive and neuropathic pain: What's the difference? - Nociceptive pain occurs in response to actual or potential tissue damage (like from a cut or arthritis), whereas neuropathic pain is due to disease or dysfunction in the nervous system itself (such as diabetic neuropathy).
Types of Pain | Pain Management Education at UCSF - Nociceptive pain arises from activation of sensory nerves by tissue damage (sharp, localized), while neuropathic pain is caused by a lesion or disease directly affecting the nervous system (often burning, shooting, or tingling).
FAQs
What is pain?
Pain is a complex sensory and emotional experience caused by actual or potential tissue damage, signaling the nervous system to protect the body.
What is the difference between nociceptive pain and neuropathic pain?
Nociceptive pain arises from actual or potential tissue damage activating pain receptors, while neuropathic pain results from injury or dysfunction in the nervous system itself.
What causes nociceptive pain?
Nociceptive pain is caused by the activation of nociceptors due to tissue injury, inflammation, or mechanical damage.
What causes neuropathic pain?
Neuropathic pain is caused by damage or dysfunction in the nervous system, including conditions such as diabetes, shingles, multiple sclerosis, nerve trauma, or spinal cord injury.
How is nociceptive pain treated?
Nociceptive pain is treated with analgesics such as nonsteroidal anti-inflammatory drugs (NSAIDs), acetaminophen, opioids, physical therapy, and addressing the underlying cause of pain.
How is neuropathic pain treated?
Neuropathic pain is treated with medications like anticonvulsants (gabapentin, pregabalin), antidepressants (duloxetine, amitriptyline), topical agents (lidocaine, capsaicin), and in some cases, opioids or nerve blocks.
Can nociceptive and neuropathic pain occur together?
Nociceptive and neuropathic pain can occur together, often described as mixed pain, commonly seen in conditions like diabetic neuropathy and cancer pain.