Root Cause Analysis (RCA) focuses on identifying the underlying causes of specific problems to prevent recurrence, while Failure Mode and Effects Analysis (FMEA) proactively evaluates potential failure modes within a system to mitigate risks. RCA is reactive and used after an issue has occurred, whereas FMEA is preventive, integrating risk assessment during design or process development stages. Explore these methodologies further to enhance quality management and operational reliability.
Main Difference
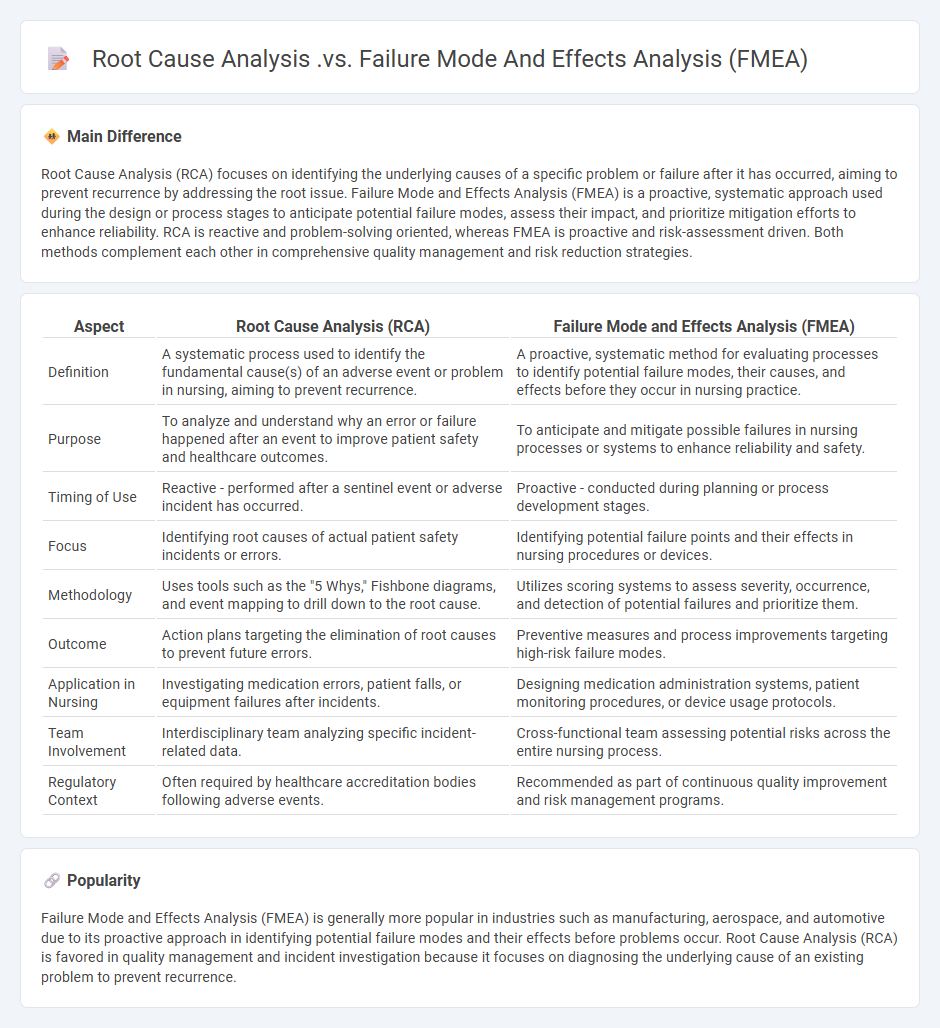
Root Cause Analysis (RCA) focuses on identifying the underlying causes of a specific problem or failure after it has occurred, aiming to prevent recurrence by addressing the root issue. Failure Mode and Effects Analysis (FMEA) is a proactive, systematic approach used during the design or process stages to anticipate potential failure modes, assess their impact, and prioritize mitigation efforts to enhance reliability. RCA is reactive and problem-solving oriented, whereas FMEA is proactive and risk-assessment driven. Both methods complement each other in comprehensive quality management and risk reduction strategies.
Connection
Root Cause Analysis (RCA) and Failure Mode and Effects Analysis (FMEA) are connected through their common goal of identifying and addressing potential failures to improve system reliability. FMEA systematically evaluates potential failure modes and their effects, providing a proactive approach, while RCA focuses on diagnosing the underlying causes of actual failures for corrective action. Together, they form a comprehensive risk management strategy by combining preventive assessment with reactive problem-solving.
Comparison Table
| Aspect | Root Cause Analysis (RCA) | Failure Mode and Effects Analysis (FMEA) |
|---|---|---|
| Definition | A systematic process used to identify the fundamental cause(s) of an adverse event or problem in nursing, aiming to prevent recurrence. | A proactive, systematic method for evaluating processes to identify potential failure modes, their causes, and effects before they occur in nursing practice. |
| Purpose | To analyze and understand why an error or failure happened after an event to improve patient safety and healthcare outcomes. | To anticipate and mitigate possible failures in nursing processes or systems to enhance reliability and safety. |
| Timing of Use | Reactive - performed after a sentinel event or adverse incident has occurred. | Proactive - conducted during planning or process development stages. |
| Focus | Identifying root causes of actual patient safety incidents or errors. | Identifying potential failure points and their effects in nursing procedures or devices. |
| Methodology | Uses tools such as the "5 Whys," Fishbone diagrams, and event mapping to drill down to the root cause. | Utilizes scoring systems to assess severity, occurrence, and detection of potential failures and prioritize them. |
| Outcome | Action plans targeting the elimination of root causes to prevent future errors. | Preventive measures and process improvements targeting high-risk failure modes. |
| Application in Nursing | Investigating medication errors, patient falls, or equipment failures after incidents. | Designing medication administration systems, patient monitoring procedures, or device usage protocols. |
| Team Involvement | Interdisciplinary team analyzing specific incident-related data. | Cross-functional team assessing potential risks across the entire nursing process. |
| Regulatory Context | Often required by healthcare accreditation bodies following adverse events. | Recommended as part of continuous quality improvement and risk management programs. |
Root Cause Analysis (RCA)
Root Cause Analysis (RCA) in nursing identifies underlying causes of patient safety incidents to prevent recurrence. RCA involves a systematic investigation led by multidisciplinary teams analyzing clinical errors, workflow deficiencies, and communication breakdowns. Techniques such as the "5 Whys" and fishbone diagrams enhance understanding of complex healthcare events. Effective RCA improves nursing practices, patient outcomes, and adherence to standards set by organizations like The Joint Commission.
Failure Mode and Effects Analysis (FMEA)
Failure Mode and Effects Analysis (FMEA) is a systematic approach used in nursing to identify potential failure points in patient care processes and assess their impact on patient safety. By analyzing possible failure modes, nursing teams can prioritize risks based on severity, occurrence, and detectability, leading to targeted interventions that reduce errors. Implementing FMEA in clinical settings enhances proactive risk management, improves care quality, and supports compliance with healthcare safety standards such as those outlined by The Joint Commission. This method promotes continuous quality improvement and fosters a culture of safety within nursing practice.
Reactive Approach vs. Proactive Approach
In nursing, a reactive approach addresses patient issues as they arise, often responding to symptoms, emergencies, or complications after they have developed. A proactive approach emphasizes prevention, early detection, and intervention, aiming to reduce risks and improve patient outcomes through ongoing assessment and education. Studies show proactive nursing care reduces hospital readmissions and improves chronic disease management, highlighting its critical role in modern healthcare. Integrating technology, such as predictive analytics and patient monitoring systems, further enhances the effectiveness of proactive nursing strategies.
Incident Investigation vs. Risk Assessment
Incident investigation in nursing involves analyzing specific adverse events to identify root causes and prevent recurrence, focusing on actual patient safety breaches and errors. Risk assessment systematically evaluates potential hazards and vulnerabilities in clinical environments to proactively mitigate risks before they cause harm, often using tools like Failure Mode and Effects Analysis (FMEA). Both processes utilize evidence-based methodologies to enhance patient outcomes, but incident investigations address past occurrences, whereas risk assessments forecast and reduce future risks. Integration of these strategies supports comprehensive clinical risk management and promotes a culture of safety in healthcare settings.
Patient Safety Improvement
Patient safety improvement in nursing focuses on implementing evidence-based practices to reduce medical errors and adverse events. Key strategies include standardized protocols, effective communication among healthcare teams, and continuous staff training on patient safety. Utilizing electronic health records and monitoring systems enhances error detection and supports timely interventions. Research indicates that hospitals adopting comprehensive patient safety programs experience significant decreases in hospital-acquired infections and medication errors.
Source and External Links
Guidance for Performing Failure Mode and Effects Analysis ... - FMEA is a structured, proactive method to identify and prevent potential failures before they occur, while RCA is a structured, reactive method to analyze and address problems after they have happened.
How are FMEA and RCA Connected? - Both FMEA and RCA are based on cause-and-effect analysis, but FMEA anticipates future failures to prevent them, whereas RCA investigates past incidents to understand why they occurred.
Root Cause Analysis (RCA) vs Failure Mode and Effect Analysis (FMEA) - RCA is reactive and aims to eliminate the root cause of a problem after it happens, focusing on corrective actions, while FMEA is proactive, identifying and prioritizing potential failure modes to implement preventive measures before problems arise.
FAQs
What is Root Cause Analysis?
Root Cause Analysis is a systematic process used to identify the fundamental causes of problems or incidents to prevent recurrence.
What is Failure Mode and Effects Analysis?
Failure Mode and Effects Analysis (FMEA) is a systematic method used to identify, evaluate, and prioritize potential failure modes in a product or process and their effects to improve reliability and safety.
How does Root Cause Analysis differ from FMEA?
Root Cause Analysis identifies the fundamental cause of an existing problem, while Failure Modes and Effects Analysis (FMEA) systematically predicts and prevents potential failures before they occur.
What are the main steps in Root Cause Analysis?
The main steps in Root Cause Analysis are: defining the problem, collecting data, identifying possible causes, analyzing the root cause, implementing corrective actions, and monitoring the results.
What are the main steps in FMEA?
Identify potential failure modes, assess their severity, occurrence, and detection, calculate risk priority numbers (RPN), prioritize failure modes based on RPN, develop and implement corrective actions, and review the effectiveness of actions taken.
When should you use Root Cause Analysis versus FMEA?
Use Root Cause Analysis (RCA) to identify and address the underlying causes of an existing problem or failure, and use Failure Modes and Effects Analysis (FMEA) proactively to predict and prevent potential failure modes and their impacts in a process or product design.
What industries rely on FMEA and Root Cause Analysis?
Automotive, aerospace, manufacturing, healthcare, electronics, and chemical industries rely heavily on FMEA and Root Cause Analysis to improve quality and safety.