SOAP Notes structure documentation into Subjective, Objective, Assessment, and Plan sections, streamlining clinical communication for healthcare providers. DAR Notes focus on Data, Action, and Response, emphasizing ongoing patient care and treatment outcomes in nursing and allied health fields. Explore detailed comparisons to understand which documentation method best suits your clinical practice.
Main Difference
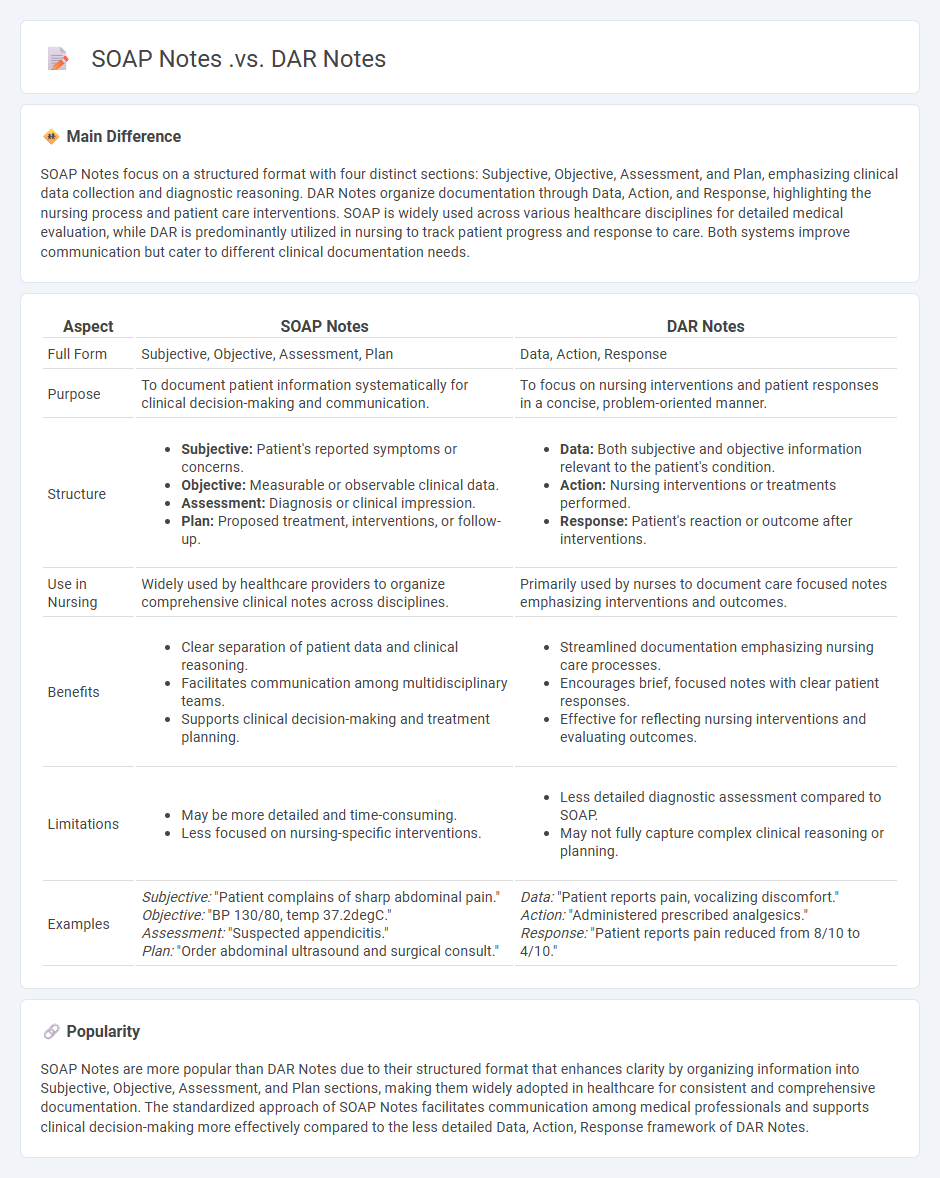
SOAP Notes focus on a structured format with four distinct sections: Subjective, Objective, Assessment, and Plan, emphasizing clinical data collection and diagnostic reasoning. DAR Notes organize documentation through Data, Action, and Response, highlighting the nursing process and patient care interventions. SOAP is widely used across various healthcare disciplines for detailed medical evaluation, while DAR is predominantly utilized in nursing to track patient progress and response to care. Both systems improve communication but cater to different clinical documentation needs.
Connection
SOAP Notes and DAR Notes both serve as structured methods for clinical documentation, enhancing communication and continuity of care. SOAP Notes organize information into Subjective, Objective, Assessment, and Plan sections, while DAR Notes focus on Data, Action, and Response to capture patient interactions more dynamically. Their interconnected use improves accuracy and efficiency in tracking patient progress and treatment outcomes.
Comparison Table
| Aspect | SOAP Notes | DAR Notes |
|---|---|---|
| Full Form | Subjective, Objective, Assessment, Plan | Data, Action, Response |
| Purpose | To document patient information systematically for clinical decision-making and communication. | To focus on nursing interventions and patient responses in a concise, problem-oriented manner. |
| Structure |
|
|
| Use in Nursing | Widely used by healthcare providers to organize comprehensive clinical notes across disciplines. | Primarily used by nurses to document care focused notes emphasizing interventions and outcomes. |
| Benefits |
|
|
| Limitations |
|
|
| Examples | Subjective: "Patient complains of sharp abdominal pain." Objective: "BP 130/80, temp 37.2degC." Assessment: "Suspected appendicitis." Plan: "Order abdominal ultrasound and surgical consult." |
Data: "Patient reports pain, vocalizing discomfort." Action: "Administered prescribed analgesics." Response: "Patient reports pain reduced from 8/10 to 4/10." |
Subjective Data
Subjective data in nursing refers to information reported directly by the patient about their experiences, feelings, and perceptions, such as pain intensity, mood, and symptoms like nausea or dizziness. This data is essential for comprehensive assessments, as it provides insight into the patient's internal conditions that cannot be measured objectively. Nurses collect subjective data through patient interviews, health histories, and verbal descriptions, ensuring a patient-centered approach to care planning. Accurate documentation of subjective data supports diagnosis, treatment decisions, and the evaluation of therapeutic outcomes.
Objective Data
Objective data in nursing refers to measurable and observable information collected through physical examination, vital signs, laboratory results, and diagnostic tests. Nurses document objective data such as temperature, blood pressure, respiratory rate, heart rate, and oxygen saturation to assess a patient's health status accurately. This data provides a factual basis for clinical decision-making and complements subjective data obtained from patient interviews. Accurate recording of objective data is essential for developing effective nursing care plans and monitoring patient progress.
Assessment
Assessment in nursing involves systematic data collection to evaluate a patient's physical, psychological, and social health status. Nurses utilize tools such as head-to-toe examinations, health history interviews, and diagnostic tests to identify actual or potential health problems. Accurate assessment supports clinical decision-making and individualized care planning, improving patient outcomes. Documentation of findings ensures continuity of care and effective communication within the healthcare team.
Focus Charting
Focus charting in nursing is a documentation method that centers on patient concerns, behaviors, and responses, promoting a holistic approach to care. It uses the DAR format--Data, Action, and Response--to systematically record clinical observations, nursing interventions, and patient outcomes. This method enhances communication among healthcare professionals by emphasizing patient-focused narratives and critical thinking. Focus charting aligns with nursing standards such as the North American Nursing Diagnosis Association (NANDA) and supports accurate, efficient, and legal documentation.
Documentation Structure
Comprehensive nursing documentation ensures accurate patient care records, legal compliance, and effective communication among healthcare providers. It includes assessments, care plans, interventions, patient responses, and discharge summaries, adhering to standards like the Joint Commission and HIPAA regulations. Electronic Health Records (EHR) systems, such as Epic and Cerner, facilitate real-time documentation, improve accuracy, and support data analysis for quality improvement. Proper nursing documentation reduces errors, enhances patient safety, and supports clinical decision-making.
Source and External Links
What's the Difference: SOAP Notes vs DAP Notes | Power Diary - SOAP notes separately record subjective and objective data, while DAP notes combine both in the Data section for quicker documentation.
Advantages of Using SRIP, SOAP, DAR, and DAP for Healthcare Professionals - SOAP notes provide thorough analysis through structured sections, whereas DAR notes (Data, Action, Response) are commonly used in nursing and focus on documenting specific interventions and patient responses.
Your Guide to Effective DARP Notes (with PDF Template) - Psylio - SOAP notes gather broad information to inform clinical treatment, while DARP notes combine data types and include a Response section to track client reactions, offering a different emphasis in clinical documentation.
FAQs
What are SOAP notes?
SOAP notes are structured medical documentation consisting of four sections: Subjective, Objective, Assessment, and Plan, used by healthcare providers to record patient information and treatment plans.
What are DAR notes?
DAR notes are daily documentation records used by healthcare professionals, summarizing the Data, Action, and Response related to a patient's care.
How do SOAP notes differ from DAR notes?
SOAP notes focus on Subjective data, Objective data, Assessment, and Plan, while DAR notes organize documentation into Data, Action, and Response categories for a more concise clinical record.
What are the main components of SOAP notes?
SOAP notes consist of four main components: Subjective, Objective, Assessment, and Plan.
What information is included in DAR notes?
DAR notes include Data (factual information or observations), Action (interventions or steps taken), and Response (patient's reaction or outcome).
When should you use SOAP notes vs. DAR notes?
Use SOAP notes for structured clinical documentation focusing on Subjective, Objective, Assessment, and Plan data; use DAR notes for narrative, behavior-focused nursing documentation organized by Data, Action, and Response.
What are the advantages of using SOAP or DAR notes?
SOAP and DAR notes improve clinical communication by structuring patient information into clear categories, enhancing documentation accuracy, supporting better diagnosis and treatment plans, facilitating continuity of care, and meeting legal and regulatory requirements.