Catatonia and mutism are neuropsychiatric conditions with distinct clinical presentations but overlapping features such as reduced speech and motor activity. Catatonia often includes symptoms like stupor, rigidity, and posturing, commonly associated with psychiatric disorders or medical conditions. Explore the key differences and diagnostic criteria to better understand these complex syndromes.
Main Difference
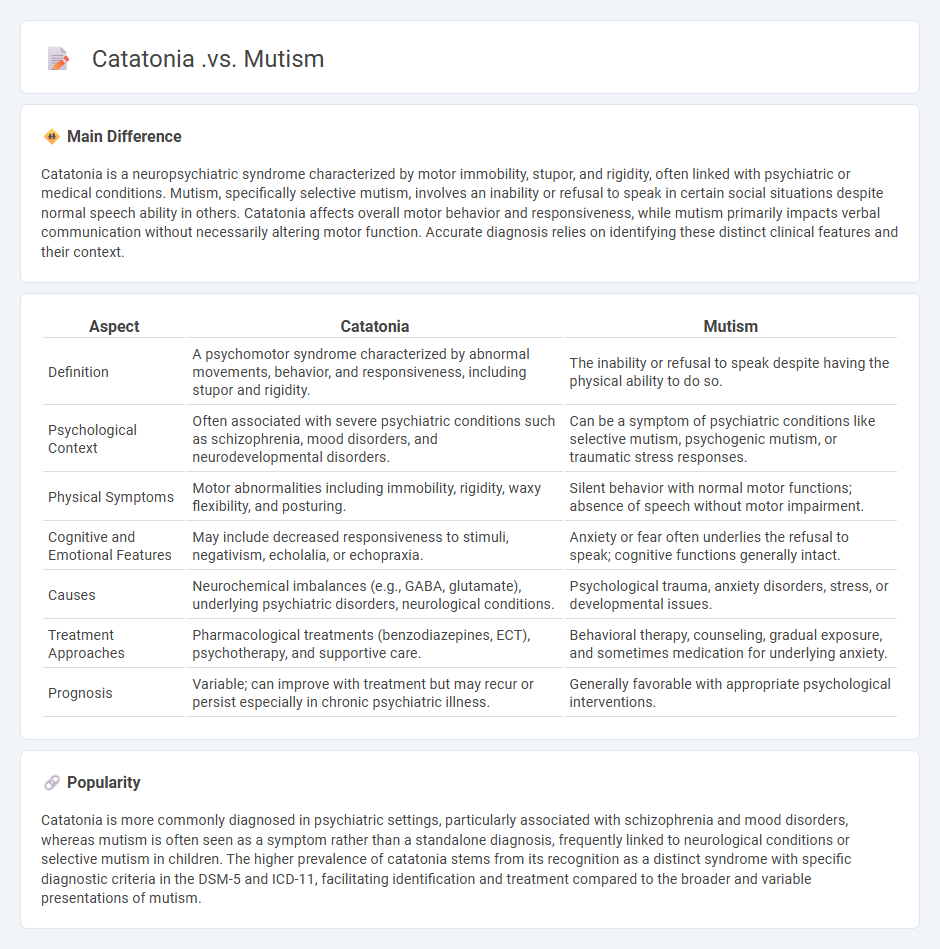
Catatonia is a neuropsychiatric syndrome characterized by motor immobility, stupor, and rigidity, often linked with psychiatric or medical conditions. Mutism, specifically selective mutism, involves an inability or refusal to speak in certain social situations despite normal speech ability in others. Catatonia affects overall motor behavior and responsiveness, while mutism primarily impacts verbal communication without necessarily altering motor function. Accurate diagnosis relies on identifying these distinct clinical features and their context.
Connection
Catatonia is a neuropsychiatric syndrome characterized by motor immobility and behavioral abnormalities, with mutism being a common symptom where the patient fails to speak despite being conscious. Both catatonia and mutism share underlying disruptions in neural circuits, particularly involving the frontal cortex and basal ganglia, which affect communication and voluntary motor functions. Understanding their connection is crucial for accurate diagnosis and effective treatment strategies, such as benzodiazepines or electroconvulsive therapy.
Comparison Table
| Aspect | Catatonia | Mutism |
|---|---|---|
| Definition | A psychomotor syndrome characterized by abnormal movements, behavior, and responsiveness, including stupor and rigidity. | The inability or refusal to speak despite having the physical ability to do so. |
| Psychological Context | Often associated with severe psychiatric conditions such as schizophrenia, mood disorders, and neurodevelopmental disorders. | Can be a symptom of psychiatric conditions like selective mutism, psychogenic mutism, or traumatic stress responses. |
| Physical Symptoms | Motor abnormalities including immobility, rigidity, waxy flexibility, and posturing. | Silent behavior with normal motor functions; absence of speech without motor impairment. |
| Cognitive and Emotional Features | May include decreased responsiveness to stimuli, negativism, echolalia, or echopraxia. | Anxiety or fear often underlies the refusal to speak; cognitive functions generally intact. |
| Causes | Neurochemical imbalances (e.g., GABA, glutamate), underlying psychiatric disorders, neurological conditions. | Psychological trauma, anxiety disorders, stress, or developmental issues. |
| Treatment Approaches | Pharmacological treatments (benzodiazepines, ECT), psychotherapy, and supportive care. | Behavioral therapy, counseling, gradual exposure, and sometimes medication for underlying anxiety. |
| Prognosis | Variable; can improve with treatment but may recur or persist especially in chronic psychiatric illness. | Generally favorable with appropriate psychological interventions. |
Motor immobility
Motor immobility in psychology refers to a state where an individual experiences a pronounced inhibition of voluntary muscle movements, often linked to extreme stress, trauma, or psychiatric conditions such as catatonia and major depressive disorder. This phenomenon is characterized by a marked reduction or complete absence of spontaneous motor activity and can be observed in both neurological and psychological contexts. Research indicates that motor immobility is associated with alterations in the brain's motor cortex, basal ganglia, and limbic system, implicating neurotransmitters like dopamine and GABA. Effective treatment commonly involves pharmacotherapy with antipsychotics or antidepressants alongside behavioral therapies aimed at restoring motor function.
Speech absence
Speech absence, also known as mutism, is a psychological condition characterized by the inability or refusal to speak in specific situations despite having the physical ability to do so. Selective mutism commonly affects children, with prevalence rates estimated at 0.1% to 0.7%, often linked to anxiety disorders such as social phobia. Treatment typically involves cognitive-behavioral therapy, emphasizing gradual exposure and social skills training to reduce anxiety and encourage verbal communication. Early intervention improves outcomes, highlighting the importance of addressing underlying psychological factors.
Psychomotor symptoms
Psychomotor symptoms in psychology refer to observable changes in motor activity and coordination often linked to mental health disorders such as depression, schizophrenia, and bipolar disorder. These symptoms include psychomotor agitation, characterized by restless movements, and psychomotor retardation, marked by slowed physical activity and speech. Neurobiological factors involving dopamine and serotonin pathways influence the expression of psychomotor symptoms, impacting the basal ganglia and prefrontal cortex. Assessment of psychomotor symptoms is critical in clinical diagnosis and treatment monitoring, utilizing scales like the Motor Agitation Scale and the Simpson-Angus Scale.
Volitional unresponsiveness
Volitional unresponsiveness refers to a psychological state in which an individual consciously refrains from reacting or engaging with stimuli despite having the capacity to respond. This phenomenon is often studied in contexts such as hypnosis, meditation, or dissociation, where volition is deliberately inhibited. Research indicates that neural pathways involved in self-control and motor inhibition, particularly within the prefrontal cortex, play a crucial role in sustaining this state. Understanding volitional unresponsiveness has implications for therapeutic interventions targeting anxiety, pain management, and behavioral modification.
Differential diagnosis
Differential diagnosis in psychology involves systematically distinguishing between mental health disorders based on symptom presentation, severity, and duration. Clinicians assess conditions such as major depressive disorder, bipolar disorder, schizophrenia, and anxiety disorders by evaluating specific diagnostic criteria outlined in the DSM-5. Accurate differential diagnosis ensures effective treatment planning by identifying comorbidities and ruling out medical or substance-induced causes. This process relies on clinical interviews, psychological testing, and collateral information to enhance diagnostic precision.
Source and External Links
Is it selective mutism--or chronic catatonia? - NeuroClastic - Catatonia can involve mutism as part of a spectrum of symptoms including freezing up, physical agitation, and an inability to speak that may overlap with selective mutism but often includes broader motor and behavioral disturbances beyond speech alone.
What Is Catatonia: Causes, Symptoms, Treatment, and More - WebMD - Catatonia is a complex syndrome featuring symptoms such as lack of movement, impaired communication (including mutism), and behavioral abnormalities, distinct from mutism which refers specifically to the inability or refusal to speak.
Catatonia and Mutism: Neurotic, Psychotic, or Organic Disorder? - PMC - While mutism may occur in catatonia, catatonia itself is a broader condition involving psychomotor impairment that can arise from psychiatric or organic causes, needing differential diagnosis to distinguish from pure mutism or other medical disorders.
FAQs
What is catatonia?
Catatonia is a neuropsychiatric syndrome characterized by motor immobility, mutism, stupor, rigidity, and abnormal movements, often associated with psychiatric disorders like schizophrenia and mood disorders.
What is mutism?
Mutism is a neurological or psychological condition characterized by an individual's inability or refusal to speak despite having the physical ability to do so.
How does catatonia differ from mutism?
Catatonia is a neuropsychiatric syndrome characterized by motor abnormalities such as stupor, rigidity, and posturing, often accompanied by mutism, whereas mutism is specifically the inability or refusal to speak without the broader motor symptoms seen in catatonia.
What are the symptoms of catatonia?
Symptoms of catatonia include motor immobility, stupor, mutism, negativism, posturing, waxy flexibility, echolalia, echopraxia, agitation, grimacing, and stereotypy.
What causes mutism?
Mutism is caused by neurological disorders, brain injuries, psychological trauma, developmental conditions such as selective mutism, and speech or language impairments.
How are catatonia and mutism diagnosed?
Catatonia is diagnosed using clinical criteria such as the Bush-Francis Catatonia Rating Scale or DSM-5 criteria, focusing on symptoms like motor immobility, stupor, or rigidity; mutism is identified through clinical observation of the absence of speech despite intact understanding, often assessed via neurological and psychiatric evaluations.
What are the treatment options for catatonia and mutism?
Treatment options for catatonia and mutism include benzodiazepines (especially lorazepam), electroconvulsive therapy (ECT), and addressing underlying medical or psychiatric conditions.