Conversion disorder involves neurological symptoms such as paralysis or blindness without a medical cause, often triggered by psychological stress, whereas somatization disorder is characterized by multiple, recurrent physical complaints across various bodily systems without identifiable organic pathology. Both disorders are classified under somatic symptom and related disorders in the DSM-5, highlighting the intricate connection between mind and body. Explore the distinctions and diagnostic criteria to better understand these complex conditions.
Main Difference
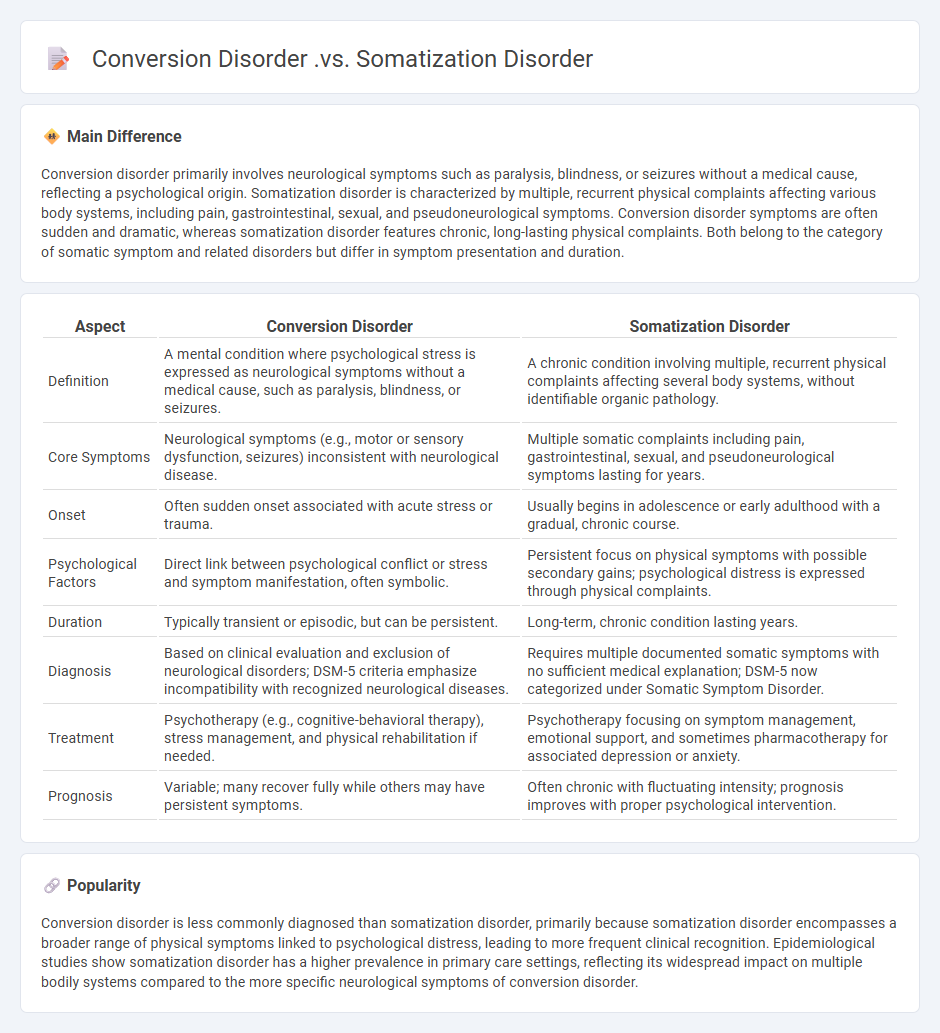
Conversion disorder primarily involves neurological symptoms such as paralysis, blindness, or seizures without a medical cause, reflecting a psychological origin. Somatization disorder is characterized by multiple, recurrent physical complaints affecting various body systems, including pain, gastrointestinal, sexual, and pseudoneurological symptoms. Conversion disorder symptoms are often sudden and dramatic, whereas somatization disorder features chronic, long-lasting physical complaints. Both belong to the category of somatic symptom and related disorders but differ in symptom presentation and duration.
Connection
Conversion disorder and somatization disorder share a close connection through their classification as somatic symptom and related disorders, characterized by the presence of physical symptoms without a fully explained medical condition. Both disorders involve the manifestation of psychological distress through bodily symptoms, with conversion disorder primarily presenting neurological symptoms like paralysis or seizures, while somatization disorder involves multiple, chronic physical complaints across various organ systems. Understanding the overlap in their symptomatology and underlying psychological mechanisms is essential for accurate diagnosis and effective psychosomatic treatment strategies.
Comparison Table
| Aspect | Conversion Disorder | Somatization Disorder |
|---|---|---|
| Definition | A mental condition where psychological stress is expressed as neurological symptoms without a medical cause, such as paralysis, blindness, or seizures. | A chronic condition involving multiple, recurrent physical complaints affecting several body systems, without identifiable organic pathology. |
| Core Symptoms | Neurological symptoms (e.g., motor or sensory dysfunction, seizures) inconsistent with neurological disease. | Multiple somatic complaints including pain, gastrointestinal, sexual, and pseudoneurological symptoms lasting for years. |
| Onset | Often sudden onset associated with acute stress or trauma. | Usually begins in adolescence or early adulthood with a gradual, chronic course. |
| Psychological Factors | Direct link between psychological conflict or stress and symptom manifestation, often symbolic. | Persistent focus on physical symptoms with possible secondary gains; psychological distress is expressed through physical complaints. |
| Duration | Typically transient or episodic, but can be persistent. | Long-term, chronic condition lasting years. |
| Diagnosis | Based on clinical evaluation and exclusion of neurological disorders; DSM-5 criteria emphasize incompatibility with recognized neurological diseases. | Requires multiple documented somatic symptoms with no sufficient medical explanation; DSM-5 now categorized under Somatic Symptom Disorder. |
| Treatment | Psychotherapy (e.g., cognitive-behavioral therapy), stress management, and physical rehabilitation if needed. | Psychotherapy focusing on symptom management, emotional support, and sometimes pharmacotherapy for associated depression or anxiety. |
| Prognosis | Variable; many recover fully while others may have persistent symptoms. | Often chronic with fluctuating intensity; prognosis improves with proper psychological intervention. |
Symptom Type: Neurological (Conversion Disorder) vs. Multiple Physical Complaints (Somatization Disorder)
Conversion disorder primarily manifests through neurological symptoms such as paralysis, blindness, or seizures without a medical cause, reflecting an unconscious psychological conflict. Somatization disorder involves multiple, recurrent physical complaints across various organ systems, including pain, gastrointestinal, sexual, and neurological symptoms, that cannot be fully explained by medical conditions. Both disorders are classified under somatic symptom and related disorders in the DSM-5, but conversion disorder emphasizes motor or sensory dysfunction, whereas somatization disorder presents with a broader spectrum of physical complaints. Effective diagnosis requires comprehensive clinical evaluation to distinguish psychological origins from physiological pathology.
Symptom Origin: Psychological Distress Expressed as Physical (Both)
Psychological distress frequently manifests as physical symptoms, a phenomenon known as somatization, where emotional pain translates into bodily discomfort such as headaches or gastrointestinal issues. Research indicates that stress, anxiety, and depression are strongly correlated with increased reports of pain and fatigue in patients, complicating diagnosis and treatment. Neurobiological studies reveal that dysregulation in the hypothalamic-pituitary-adrenal (HPA) axis and heightened inflammatory markers contribute to the physical presentation of psychological distress. Effective management requires integrated care combining psychological therapy, such as cognitive-behavioral therapy (CBT), with medical interventions to address both mental and somatic symptoms.
Diagnostic Criteria: Specific Functional Deficits (Conversion) vs. Variety of Symptoms Across Organ Systems (Somatization)
Conversion disorder is characterized by specific functional neurological symptoms such as paralysis, blindness, or seizures that cannot be explained by medical conditions but are linked to psychological factors. Somatization disorder presents a wide range of physical symptoms affecting multiple organ systems, including pain, gastrointestinal, sexual, and pseudoneurological symptoms, without a clear medical cause. The DSM-5 highlights that conversion symptoms are typically sudden and sensory or motor in nature, whereas somatization symptoms are chronic and diverse, often leading to extensive medical evaluations. Accurate diagnosis relies on distinguishing these symptom patterns by thorough clinical assessment and ruling out organic pathology.
Conscious Control: Symptoms Unintentional (Both)
Conscious control over unintentional symptoms often involves the ability to recognize and modulate involuntary behaviors, such as tics or muscle spasms, commonly studied in clinical psychology. Disorders like Tourette Syndrome or psychogenic movement disorders highlight the complexity of distinguishing between voluntary and involuntary symptom expression. Therapeutic approaches focus on increasing patient awareness and employing cognitive-behavioral techniques to reduce symptom frequency and severity. Neuroimaging studies reveal differential activation patterns in brain regions such as the supplementary motor area and prefrontal cortex during conscious attempts to suppress involuntary symptoms.
Duration and Pattern: Acute Onset (Conversion) vs. Chronic Course (Somatization)
Acute onset conversion disorder typically manifests suddenly, with dramatic neurological symptoms such as paralysis or blindness that lack a medical explanation, often triggered by psychological stress. In contrast, somatization disorder presents a chronic course, characterized by multiple, recurrent physical complaints--such as pain, gastrointestinal issues, and fatigue--that persist over years and lead to significant impairment. Conversion symptoms are often transient and fluctuate in intensity, whereas somatization involves enduring symptoms that affect various bodily systems. Understanding these patterns aids clinicians in differential diagnosis and guides appropriate therapeutic interventions.
Source and External Links
Conversion Disorder vs. Somatic Symptom Disorder Explained - Both disorders involve mental distress manifesting as physical symptoms, but conversion disorder is characterized by neurological symptoms (like blindness or paralysis), while somatic symptom disorder typically involves physical pain or discomfort not explained by a medical condition.
Somatization and Conversion Disorder - Sage Journals - Somatization is the expression of psychological distress as physical symptoms, often linked to mood disorders, whereas conversion disorder specifically involves symptoms affecting the voluntary nervous system, such as paralysis or seizures, without an organic cause.
Conversion Disorder: What It Is, Causes, Symptoms & Treatment - Conversion disorder causes real, uncontrollable physical symptoms related to brain function (e.g., movement or sensory issues), while somatic symptom disorder is marked by distressing physical symptoms accompanied by excessive thoughts, feelings, or behaviors about those symptoms.
FAQs
What is conversion disorder?
Conversion disorder is a mental health condition characterized by neurological symptoms like paralysis, blindness, or seizures without a physiological cause, often linked to psychological stress.
What is somatization disorder?
Somatization disorder is a chronic psychological condition characterized by multiple, recurrent physical symptoms without a detectable medical cause, leading to significant distress and impairment.
How do the symptoms of conversion disorder differ from somatization disorder?
Conversion disorder symptoms involve neurological deficits like paralysis or blindness without medical cause, while somatization disorder presents multiple, recurring physical complaints across various organ systems without identifiable organic pathology.
What causes conversion disorder?
Conversion disorder is caused by psychological stress or trauma triggering neurological symptoms without a medical explanation.
What causes somatization disorder?
Somatization disorder is caused by a combination of genetic factors, psychological stress, childhood trauma, and dysfunctional coping mechanisms.
How are conversion disorder and somatization disorder diagnosed?
Conversion disorder is diagnosed based on neurological symptoms incompatible with medical conditions after thorough clinical evaluation and exclusion of neurological diseases; somatization disorder is diagnosed through the presence of multiple, recurrent, medically unexplained physical symptoms spanning various organ systems over several years, following DSM-5 or ICD-10 criteria.
What are the key treatments for each disorder?
Cognitive-behavioral therapy (CBT) for anxiety disorders, SSRIs and SNRIs for depression, antipsychotics and mood stabilizers for schizophrenia and bipolar disorder, exposure therapy for PTSD, and stimulants such as methylphenidate for ADHD.