S2 and S3 heart sounds differ in timing and clinical significance, with S2 marking the closure of the aortic and pulmonary valves during end of systole and S3 occurring shortly after, indicating rapid ventricular filling phase. The presence of an S3 sound, often termed a "ventricular gallop," can suggest heart failure or increased cardiac filling pressures in adults. Explore further to understand diagnostic implications and auscultation techniques for these heart sounds.
Main Difference
The S2 heart sound, caused by the closure of the aortic and pulmonary valves, marks the end of ventricular systole and the beginning of diastole. The S3 heart sound occurs during early diastole, resulting from rapid ventricular filling and is often linked to increased atrial pressure or reduced ventricular compliance. S2 is a normal physiological sound heard in all healthy adults, while the presence of S3 may indicate pathological conditions such as heart failure or volume overload. The timing and genesis of S2 and S3 differentiate them clearly in cardiac auscultation.
Connection
S2 and S3 heart sounds are connected through the cardiac cycle, with S2 marking the closure of the aortic and pulmonary valves signaling the end of systole, and S3 occurring early in diastole due to rapid ventricular filling. The presence of S3 can indicate increased ventricular filling pressures or altered ventricular compliance, often associated with heart failure or volume overload conditions. Understanding the timing and characteristics of S2 and S3 helps in diagnosing cardiac function abnormalities and guiding clinical management.
Comparison Table
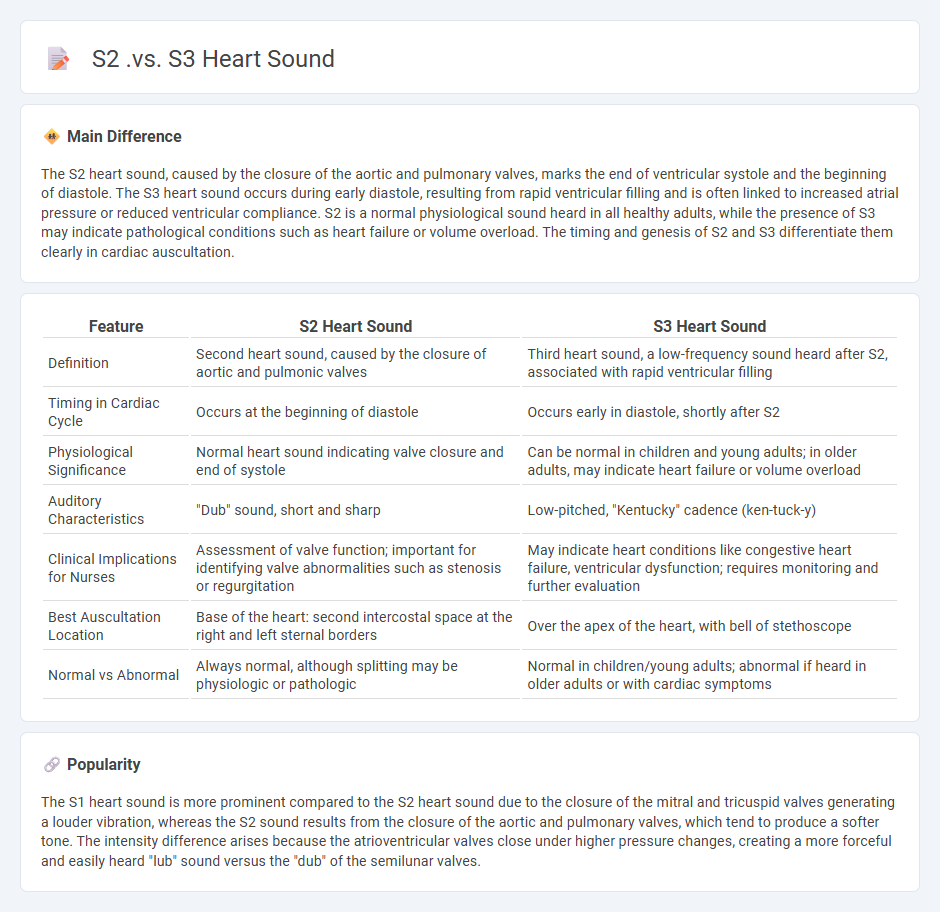
| Feature | S2 Heart Sound | S3 Heart Sound |
|---|---|---|
| Definition | Second heart sound, caused by the closure of aortic and pulmonic valves | Third heart sound, a low-frequency sound heard after S2, associated with rapid ventricular filling |
| Timing in Cardiac Cycle | Occurs at the beginning of diastole | Occurs early in diastole, shortly after S2 |
| Physiological Significance | Normal heart sound indicating valve closure and end of systole | Can be normal in children and young adults; in older adults, may indicate heart failure or volume overload |
| Auditory Characteristics | "Dub" sound, short and sharp | Low-pitched, "Kentucky" cadence (ken-tuck-y) |
| Clinical Implications for Nurses | Assessment of valve function; important for identifying valve abnormalities such as stenosis or regurgitation | May indicate heart conditions like congestive heart failure, ventricular dysfunction; requires monitoring and further evaluation |
| Best Auscultation Location | Base of the heart: second intercostal space at the right and left sternal borders | Over the apex of the heart, with bell of stethoscope |
| Normal vs Abnormal | Always normal, although splitting may be physiologic or pathologic | Normal in children/young adults; abnormal if heard in older adults or with cardiac symptoms |
Physiological Heart Sounds
Physiological heart sounds consist primarily of the first (S1) and second (S2) heart sounds, created by the closure of the atrioventricular and semilunar valves respectively. S1 sounds coincide with the onset of ventricular systole, while S2 marks the beginning of ventricular diastole. Normal heart sound auscultation is vital in nursing assessments to detect underlying cardiac function and potential abnormalities. Accurate interpretation of these sounds supports early diagnosis and effective patient management.
Timing in Cardiac Cycle
Timing in the cardiac cycle refers to the sequence of electrical and mechanical events that occur during one heartbeat, including systole and diastole phases. Systole involves ventricular contraction, ejecting blood into the aorta and pulmonary artery, while diastole is the relaxation phase allowing ventricular filling. Accurate knowledge of heart sounds--S1 and S2--helps nurses assess valve function and cardiac rhythm. Monitoring these events is crucial for evaluating cardiac output and detecting abnormalities such as arrhythmias or valve disorders.
Causes and Mechanisms
Causes and mechanisms in nursing focus on understanding the underlying factors and biological processes that contribute to health conditions and diseases. Identifying etiological agents such as pathogens, genetic mutations, environmental exposures, and lifestyle factors helps nurses tailor effective care plans. Mechanisms of disease progression often involve inflammation, cellular damage, immune responses, and metabolic imbalances, which influence symptom manifestation and treatment strategies. Knowledge of these causes and mechanisms enables nurses to provide evidence-based interventions and improve patient outcomes across diverse healthcare settings.
Clinical Significance
Clinical significance in nursing refers to the practical importance of research findings or treatment effects in patient care, beyond mere statistical significance. It emphasizes outcomes that meaningfully improve patient health, such as reduced symptom severity, enhanced quality of life, or faster recovery times. Nurses rely on clinically significant evidence to guide interventions, ensure effective care plans, and improve patient safety. Integrating clinical significance with evidence-based practice enhances decision-making and promotes optimal health outcomes.
Auscultation Locations
Key auscultation locations in nursing include the aortic valve area at the second right intercostal space, pulmonary valve area at the second left intercostal space, tricuspid valve area near the lower left sternal border, and mitral valve area at the fifth intercostal space at the midclavicular line. Nurses use the diaphragm and bell of the stethoscope to assess heart sounds, murmurs, and abnormal rhythms effectively. Accurate auscultation allows early detection of cardiac anomalies such as valve stenosis, regurgitation, or heart failure signs. Mastery of these auscultation points enhances cardiovascular assessment and patient outcomes in clinical practice.
Source and External Links
S3 heart sound: Definition, treatment, and more - Medical News Today - The S2 heart sound is a high-pitched sound caused by the closing of the aortic and pulmonic valves at the beginning of diastole, while the S3 heart sound is a low, dull sound that occurs immediately after S2 due to rapid passive filling of the left ventricle; S3 can be normal in some individuals but may also indicate heart failure or ventricular dysfunction.
Everything Med Students Need to Know About S1, S2, S3, & S4 ... - S2 marks the closure of the aortic (A2) and pulmonic (P2) valves with a split sound that varies with respiration, whereas S3 is a low-frequency sound heard after S2 during early diastole caused by rapid ventricular filling, often referred to as a ventricular gallop.
Heart sounds for beginners S1, S2, S3 & S4 #heartsounds - YouTube - The second heart sound (S2) results from pulmonary and aortic valve closure and is high-pitched, while the S3 is a low-frequency sound heard best at the apex in early diastole, caused by rapid ventricular filling, and can be physiological in young healthy people or pathological in heart disease.
FAQs
What is a heart sound?
A heart sound is the noise generated by the closing of heart valves during the cardiac cycle, primarily identified as "lub" (S1) and "dub" (S2).
What is the difference between S2 and S3 heart sounds?
S2 heart sound marks aortic and pulmonary valve closure signaling the end of systole, while S3 heart sound occurs during early diastole indicating rapid ventricular filling.
When does the S2 heart sound occur?
The S2 heart sound occurs at the closure of the aortic and pulmonary valves during the end of ventricular systole.
What causes the S3 heart sound?
The S3 heart sound is caused by rapid ventricular filling during early diastole, often associated with increased blood volume or decreased ventricular compliance.
What do the S2 and S3 heart sounds indicate about heart function?
The S2 heart sound indicates the closure of the aortic and pulmonary valves signaling the end of systole, while the S3 heart sound reflects rapid ventricular filling during early diastole, often associated with increased ventricular filling pressures or heart failure.
How are S2 and S3 heart sounds detected during examination?
S2 and S3 heart sounds are detected using a stethoscope placed at specific chest auscultation points: S2 is best heard at the base of the heart (aortic and pulmonic areas), while S3 is typically heard at the apex with the patient in the left lateral decubitus position.
Why is it important to distinguish between S2 and S3 heart sounds?
Distinguishing between S2 and S3 heart sounds is important because S2 indicates normal closure of aortic and pulmonary valves reflecting heart cycle phases, while S3 often signals abnormal ventricular filling due to heart failure or volume overload conditions.