SBAR (Situation, Background, Assessment, Recommendation) and SOAP (Subjective, Objective, Assessment, Plan) are structured communication tools used primarily in healthcare settings to enhance clarity and efficiency. SBAR focuses on concise information exchange during urgent situations, while SOAP provides a comprehensive framework for documenting patient encounters and clinical reasoning. Explore the detailed differences and applications of SBAR versus SOAP to improve communication strategies in medical practice.
Main Difference
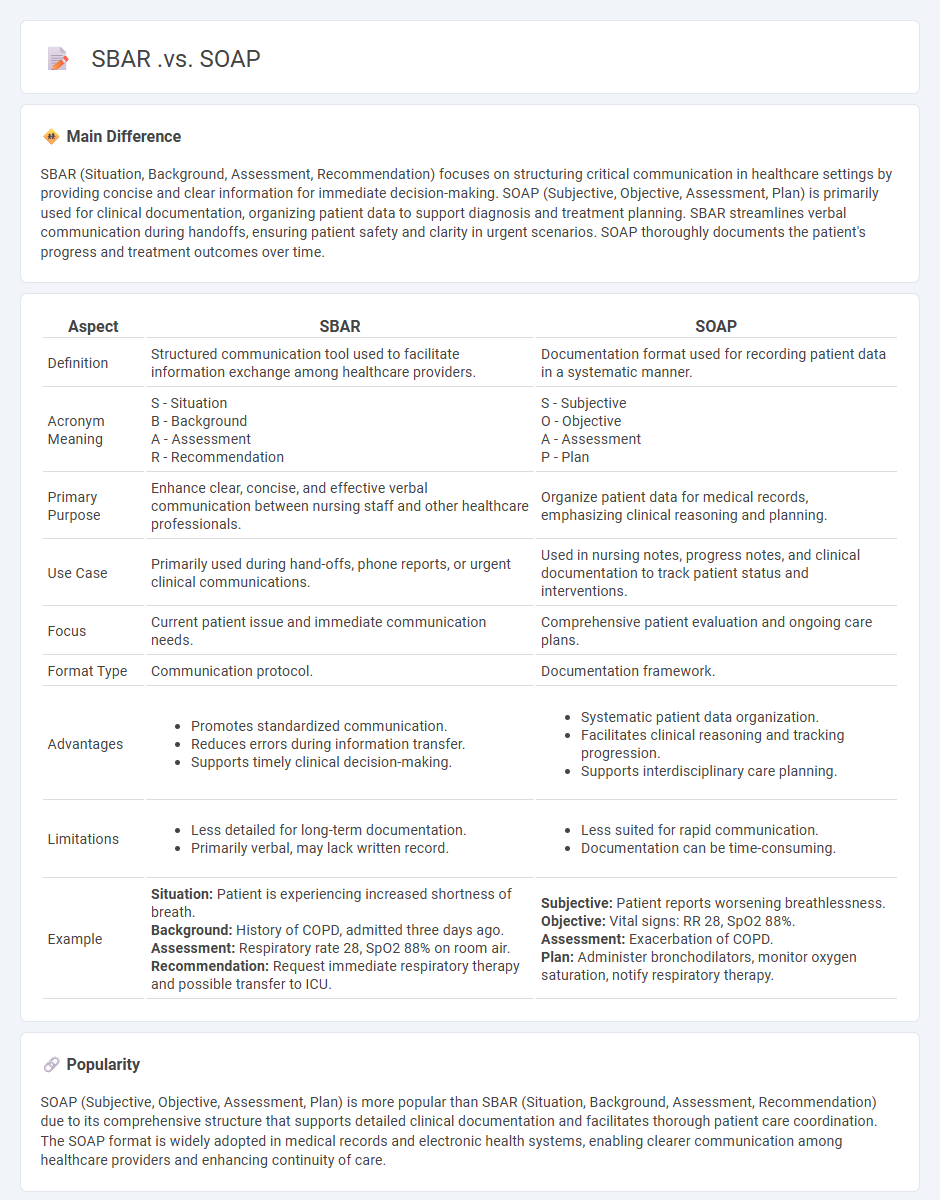
SBAR (Situation, Background, Assessment, Recommendation) focuses on structuring critical communication in healthcare settings by providing concise and clear information for immediate decision-making. SOAP (Subjective, Objective, Assessment, Plan) is primarily used for clinical documentation, organizing patient data to support diagnosis and treatment planning. SBAR streamlines verbal communication during handoffs, ensuring patient safety and clarity in urgent scenarios. SOAP thoroughly documents the patient's progress and treatment outcomes over time.
Connection
SBAR (Situation, Background, Assessment, Recommendation) and SOAP (Subjective, Objective, Assessment, Plan) are structured communication tools used in healthcare to enhance information exchange and clinical decision-making. Both frameworks emphasize assessment to facilitate accurate diagnosis and care planning, integrating subjective and objective patient data. Their complementary use improves interdisciplinary communication and patient safety in clinical settings.
Comparison Table
| Aspect | SBAR | SOAP |
|---|---|---|
| Definition | Structured communication tool used to facilitate information exchange among healthcare providers. | Documentation format used for recording patient data in a systematic manner. |
| Acronym Meaning | S - Situation B - Background A - Assessment R - Recommendation |
S - Subjective O - Objective A - Assessment P - Plan |
| Primary Purpose | Enhance clear, concise, and effective verbal communication between nursing staff and other healthcare professionals. | Organize patient data for medical records, emphasizing clinical reasoning and planning. |
| Use Case | Primarily used during hand-offs, phone reports, or urgent clinical communications. | Used in nursing notes, progress notes, and clinical documentation to track patient status and interventions. |
| Focus | Current patient issue and immediate communication needs. | Comprehensive patient evaluation and ongoing care plans. |
| Format Type | Communication protocol. | Documentation framework. |
| Advantages |
|
|
| Limitations |
|
|
| Example |
Situation: Patient is experiencing increased shortness of breath. Background: History of COPD, admitted three days ago. Assessment: Respiratory rate 28, SpO2 88% on room air. Recommendation: Request immediate respiratory therapy and possible transfer to ICU. |
Subjective: Patient reports worsening breathlessness. Objective: Vital signs: RR 28, SpO2 88%. Assessment: Exacerbation of COPD. Plan: Administer bronchodilators, monitor oxygen saturation, notify respiratory therapy. |
Structured Communication
Structured communication in nursing enhances patient safety by standardizing information exchange among healthcare professionals through tools like SBAR (Situation, Background, Assessment, Recommendation). This method reduces errors, improves clarity in critical situations, and promotes teamwork during patient handoffs. Studies show that employing structured communication protocols can decrease adverse events by up to 30%. Integration of electronic health records with communication frameworks further supports consistent and accurate data sharing across multidisciplinary teams.
Situation-Background-Assessment-Recommendation (SBAR)
Situation-Background-Assessment-Recommendation (SBAR) is a structured communication framework widely used in nursing to enhance patient safety and care coordination. Nurses employ SBAR to convey critical information clearly and efficiently during handoffs or emergencies, ensuring accurate understanding among healthcare teams. The framework consists of four components: Situation, which describes the current issue; Background, providing relevant patient history; Assessment, detailing clinical findings; and Recommendation, suggesting the next steps. Implementing SBAR has been shown to reduce communication errors and improve clinical outcomes in various healthcare settings.
Subjective-Objective-Assessment-Plan (SOAP)
The Subjective-Objective-Assessment-Plan (SOAP) format is a critical documentation method used in nursing to organize patient information systematically. Subjective data includes the patient's reported symptoms and feelings, while objective data encompasses measurable and observable findings such as vital signs and physical examination results. The assessment phase involves synthesizing subjective and objective data to formulate nursing diagnoses or clinical impressions. The plan outlines specific nursing interventions, treatments, and follow-up strategies tailored to the patient's condition and care goals.
Clinical Handover
Clinical handover in nursing ensures the accurate and efficient transfer of patient information between healthcare professionals during shift changes or care transitions. Effective communication during handover reduces medical errors and improves patient safety by maintaining continuity of care. Structured tools such as SBAR (Situation, Background, Assessment, Recommendation) enhance clarity and consistency in information exchange. Evidence shows that standardized handover protocols contribute to better clinical outcomes and increased nurse satisfaction.
Patient Safety
Patient safety in nursing is critical for reducing medical errors and preventing adverse events in healthcare settings. Implementing evidence-based protocols and adhering to standardized procedures improves care quality and minimizes risks. Continuous training and use of technology such as electronic health records (EHR) enhance communication among healthcare teams and support accurate patient monitoring. According to the World Health Organization, improving patient safety practices can significantly decrease hospital-acquired infections and medication errors.
Source and External Links
SBAR vs. SOAP: Nursing Report Templates Compared - SBAR is primarily used for verbal or written communication to give a quick report, focusing on Situation, Background, Assessment, and Recommendation, while SOAP is a structured template used mostly for documentation with Subjective, Objective, Assessment, and Plan sections.
Definitions of SBAR and SOAP | Open-i - SBAR stands for Situation, Background, Assessment, and Recommendations, and is a communication tool, whereas SOAP stands for Subjective, Objective, Assessment, and Plan, commonly used in medical notes.
SOAP vs SBAR - The key difference is that SOAP is designed for thorough note-writing, organizing patient information systematically, while SBAR provides a concise format for communicating urgent or important clinical information effectively.
FAQs
What is SBAR in healthcare communication?
SBAR in healthcare communication stands for Situation, Background, Assessment, and Recommendation, a structured method for concise and effective information exchange among medical professionals.
What does SOAP stand for in medical documentation?
SOAP stands for Subjective, Objective, Assessment, and Plan in medical documentation.
What are the main differences between SBAR and SOAP?
SBAR (Situation, Background, Assessment, Recommendation) focuses on structured communication for concise, clear handoffs, primarily in clinical or urgent contexts; SOAP (Subjective, Objective, Assessment, Plan) centers on comprehensive clinical documentation, combining patient-reported data and clinical findings to guide diagnosis and treatment planning.
When should SBAR be used instead of SOAP?
SBAR should be used instead of SOAP during urgent or critical communications to provide a clear, concise, and structured handoff or briefing between healthcare providers.
How does SBAR structure improve patient safety?
SBAR structure improves patient safety by enhancing clear, concise communication among healthcare providers, reducing misunderstandings, and ensuring critical information is accurately conveyed during patient handoffs and emergencies.
What are the advantages of using the SOAP format?
SOAP provides platform-independent communication, built-in error handling, extensibility through headers, strong security via WS-Security, and supports complex operations with standardized XML messaging.
Which format is more effective for interdisciplinary communication?
A structured format combining visual elements like flowcharts with concise textual summaries enhances interdisciplinary communication by improving clarity and shared understanding.