Pulse deficit measures the difference between the heart rate and the peripheral pulse rate, indicating possible cardiac arrhythmias or impaired blood flow. Pulse pressure, defined as the numerical difference between systolic and diastolic blood pressure, reflects arterial stiffness and cardiovascular risk. Explore detailed insights to better understand their clinical significance.
Main Difference
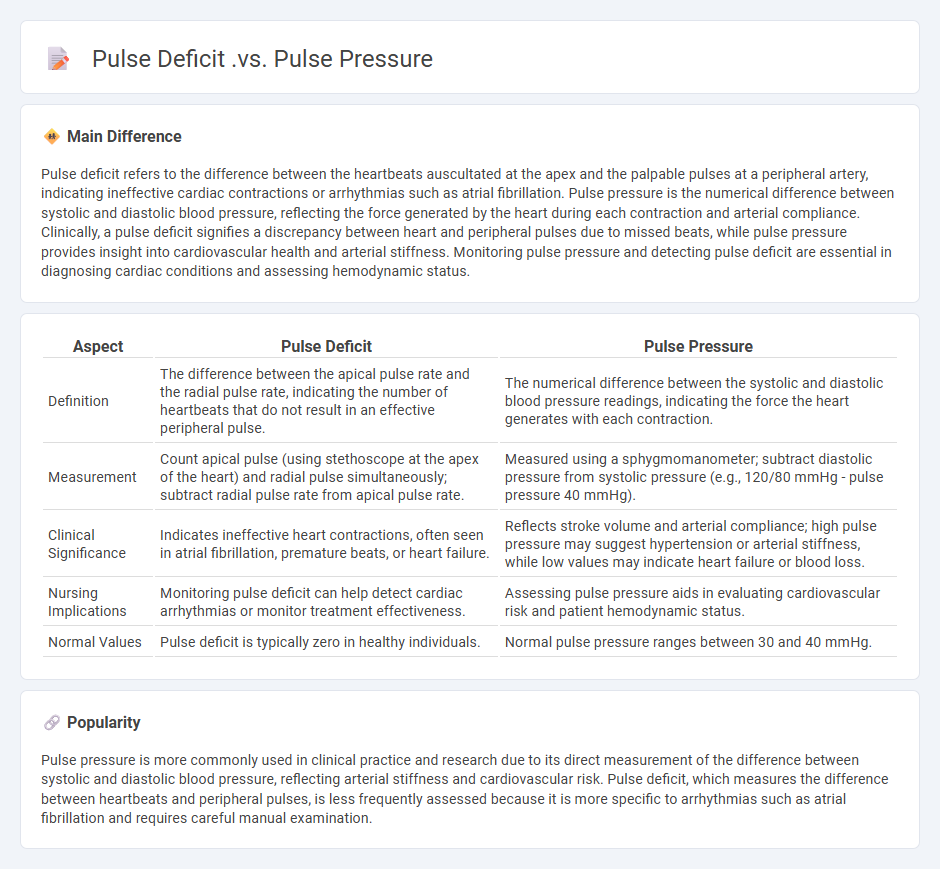
Pulse deficit refers to the difference between the heartbeats auscultated at the apex and the palpable pulses at a peripheral artery, indicating ineffective cardiac contractions or arrhythmias such as atrial fibrillation. Pulse pressure is the numerical difference between systolic and diastolic blood pressure, reflecting the force generated by the heart during each contraction and arterial compliance. Clinically, a pulse deficit signifies a discrepancy between heart and peripheral pulses due to missed beats, while pulse pressure provides insight into cardiovascular health and arterial stiffness. Monitoring pulse pressure and detecting pulse deficit are essential in diagnosing cardiac conditions and assessing hemodynamic status.
Connection
Pulse deficit, the difference between apical and radial pulse rates, often indicates irregular heart rhythms such as atrial fibrillation. Pulse pressure, calculated as the difference between systolic and diastolic blood pressure, reflects the force the heart generates each time it contracts and can influence stroke volume. Both parameters are connected through their relationship with cardiac output and arterial function, where abnormalities in pulse pressure may contribute to pulse deficit by affecting peripheral pulse transmission.
Comparison Table
| Aspect | Pulse Deficit | Pulse Pressure |
|---|---|---|
| Definition | The difference between the apical pulse rate and the radial pulse rate, indicating the number of heartbeats that do not result in an effective peripheral pulse. | The numerical difference between the systolic and diastolic blood pressure readings, indicating the force the heart generates with each contraction. |
| Measurement | Count apical pulse (using stethoscope at the apex of the heart) and radial pulse simultaneously; subtract radial pulse rate from apical pulse rate. | Measured using a sphygmomanometer; subtract diastolic pressure from systolic pressure (e.g., 120/80 mmHg - pulse pressure 40 mmHg). |
| Clinical Significance | Indicates ineffective heart contractions, often seen in atrial fibrillation, premature beats, or heart failure. | Reflects stroke volume and arterial compliance; high pulse pressure may suggest hypertension or arterial stiffness, while low values may indicate heart failure or blood loss. |
| Nursing Implications | Monitoring pulse deficit can help detect cardiac arrhythmias or monitor treatment effectiveness. | Assessing pulse pressure aids in evaluating cardiovascular risk and patient hemodynamic status. |
| Normal Values | Pulse deficit is typically zero in healthy individuals. | Normal pulse pressure ranges between 30 and 40 mmHg. |
Pulse Deficit
Pulse deficit occurs when there is a difference between the apical heart rate and the radial pulse rate, indicating ineffective cardiac contractions. It is commonly measured by simultaneously counting the apical pulse via stethoscope and radial pulse by palpation, typically over one full minute. Pulse deficit is a critical sign in conditions such as atrial fibrillation, heart failure, and other arrhythmias, where some heartbeats do not result in effective peripheral circulation. Accurate detection aids nurses in assessing cardiac function and guiding appropriate clinical interventions.
Pulse Pressure
Pulse pressure, calculated as the difference between systolic and diastolic blood pressure, serves as a key indicator in nursing for assessing cardiovascular health. Normal pulse pressure ranges from 30 to 40 mmHg, with values consistently above 60 mmHg linked to an increased risk of heart disease and arterial stiffness. Nurses monitor pulse pressure to evaluate cardiac output and detect conditions like atherosclerosis or heart failure. Accurate measurement supports timely interventions and improves patient outcomes in clinical settings.
Cardiac Output
Cardiac output (CO) is a critical physiological parameter in nursing, representing the volume of blood the heart pumps per minute, typically measured in liters per minute (L/min). It is calculated by multiplying stroke volume (SV) by heart rate (HR), with a normal adult range between 4 to 8 L/min to ensure adequate tissue perfusion. Accurate assessment of cardiac output guides clinical interventions in patients with heart failure, shock, and other cardiovascular conditions. Monitoring methods include invasive techniques like pulmonary artery catheterization and non-invasive options such as echocardiography and impedance cardiography.
Atrial Fibrillation
Atrial fibrillation (AFib) is the most common cardiac arrhythmia encountered in nursing practice, affecting approximately 2.7 to 6.1 million adults in the United States. It is characterized by an irregular and often rapid heart rate originating from disorganized atrial electrical activity, increasing the risk of stroke by fivefold. Nursing interventions focus on rate control, anticoagulation management to prevent thromboembolism, and patient education regarding symptom monitoring and lifestyle modifications. Continuous electrocardiogram (ECG) monitoring and adherence to guidelines from the American Heart Association (AHA) are essential components of optimal AFib care in clinical settings.
Hemodynamic Assessment
Hemodynamic assessment in nursing involves evaluating cardiovascular function to monitor blood flow and tissue perfusion. Nurses use invasive methods like arterial lines and central venous catheters alongside non-invasive tools such as blood pressure monitors and pulse oximetry. Key parameters assessed include cardiac output, central venous pressure, and systemic vascular resistance to detect conditions like shock or heart failure. Accurate hemodynamic monitoring guides fluid management, medication adjustments, and critical care interventions to optimize patient outcomes.
Source and External Links
Pulse Deficit | Definition, Calculation & Causes - Lesson - Pulse deficit is the difference between the apical heart rate (heartbeats heard at the apex) and the peripheral palpable pulse rate, indicating some heartbeats do not generate a peripheral pulse, often due to arrhythmias like atrial fibrillation.
Pulse Pressure: What It Means & How To Calculate It - Pulse pressure is the numerical difference between systolic and diastolic blood pressure values, reflecting the force generated by the heart during each contraction and arterial compliance; abnormal values indicate cardiovascular risks.
Pulse pressure - Pulse pressure is the difference between systolic and diastolic blood pressure, with low pulse pressure indicating conditions like low stroke volume or aortic stenosis and high pulse pressure associated with arterial stiffness and increased cardiac risk.
FAQs
What is pulse deficit?
Pulse deficit is the difference between the apical heart rate and the radial pulse rate, often indicating cardiac arrhythmias like atrial fibrillation.
What is pulse pressure?
Pulse pressure is the difference between systolic and diastolic blood pressure, indicating the force the heart generates with each contraction.
How is pulse deficit measured?
Pulse deficit is measured by simultaneously counting the apical heart rate using a stethoscope at the chest and the peripheral pulse rate at a radial artery site; the difference between the apical rate and the palpable peripheral pulse rate represents the pulse deficit.
How is pulse pressure calculated?
Pulse pressure is calculated by subtracting diastolic blood pressure from systolic blood pressure (Pulse Pressure = Systolic BP - Diastolic BP).
What causes a pulse deficit?
A pulse deficit is caused by a difference between the heartbeats heard at the apex and the palpable pulses at the peripheral arteries, often due to atrial fibrillation, premature beats, or heart failure leading to ineffective ventricular contractions.
What conditions affect pulse pressure?
Pulse pressure is affected by conditions such as atherosclerosis, arterial stiffness, hypertension, anemia, and heart valve disorders.
Why are pulse deficit and pulse pressure clinically important?
Pulse deficit helps detect atrial fibrillation indicating cardiac arrhythmia, while pulse pressure indicates arterial stiffness and cardiovascular risk.